
January 2023 – Presented by Dr. Jasper X. Zheng (Mentored by Dr. Elham Vali Betts)
Q: Seventy-one years old female with a past medical history of hypertension, rheumatoid arthritis, breast cancer (treated), and deep vein thrombosis was referred to the oral and maxillofacial department for assessment and management of a 20-mm tender nonindurated ulcer of the left lingual sulcular mucosa.
Three months prior, patient was seen by general medical practitioner who prescribed her with antifungal medication, however, the sore persisted. Her medications included bisoprolol, spironolactone, losartan, furosemide, folic acid, anastrozole, warfarin, and methotrexate (MTX). Patient denies any tobacco or alcohol usage.
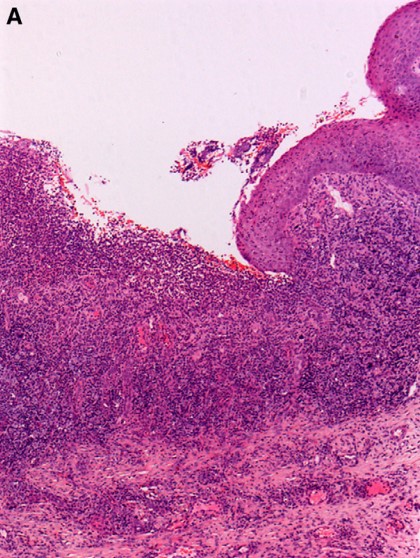
A biopsy was obtained from the ulcer shown in photomicrographs.
 Source: Attard AA, et. al., doi: 10.1016/j.oooo.2012.04.003. PMID: 22769419.
Source: Attard AA, et. al., doi: 10.1016/j.oooo.2012.04.003. PMID: 22769419.
Figure A: Biopsy of the 20-mm left lingual sulcular mucosa ulcer, Hematoxylin & Eosin at original magnification of 5x
 Source: WHO 5th edition
Source: WHO 5th edition
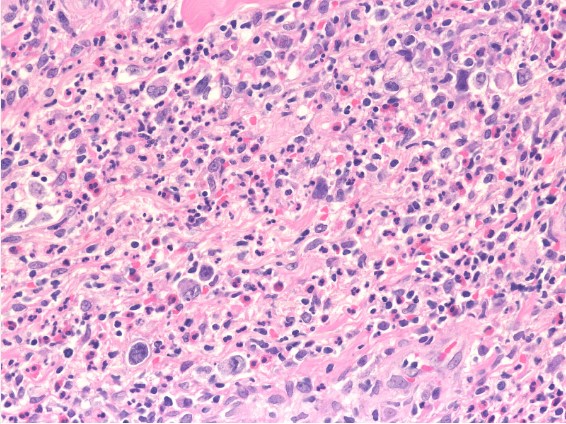
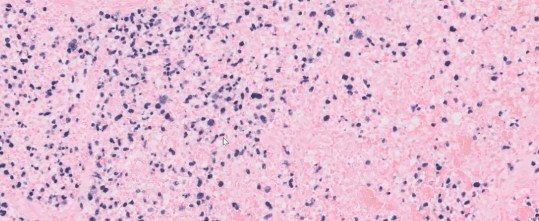
Figure B: Ulcer base demonstrating the presence of polymorphous inflammatory infiltrate including atypical large immunoblasts and Hodgkin/ Reed Sternberg-like cells, Hematoxylin & Eosin at original magnification of 400x
 Source: WHO 5th edition
Source: WHO 5th edition
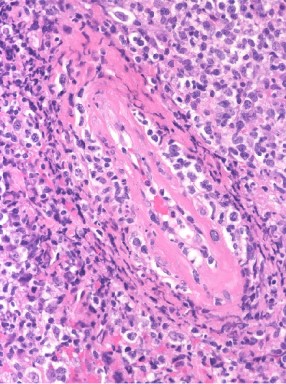
Figure C: Presence of angioinvasion by various sized lymphoid infiltrates, Hematoxylin & Eosin at original magnification of 400x
Immunohistochemical staining revealed:
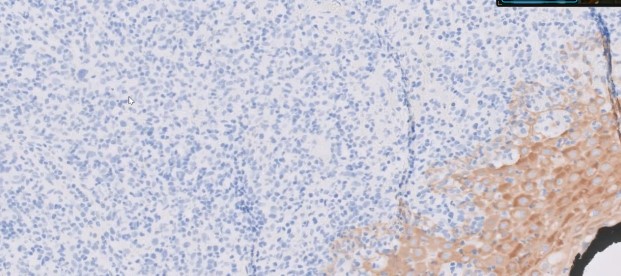 AE1/3 is negative in the hematolymphoid cells.
AE1/3 is negative in the hematolymphoid cells.
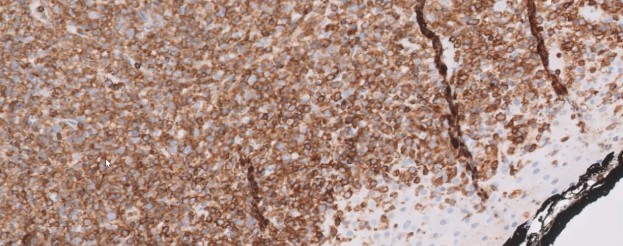 CD45
CD45
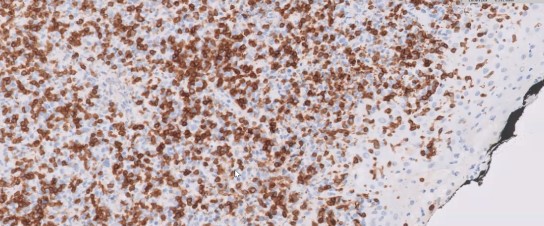 CD3
CD3
 CD20
CD20
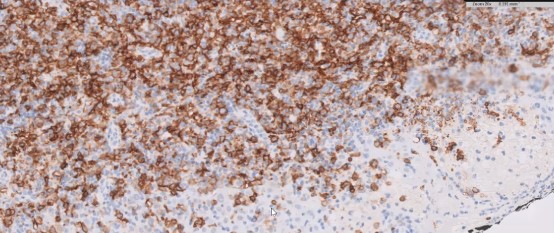
 CD15
CD15
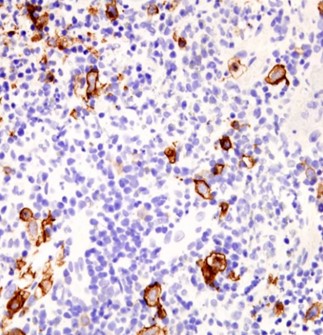 CD30
CD30
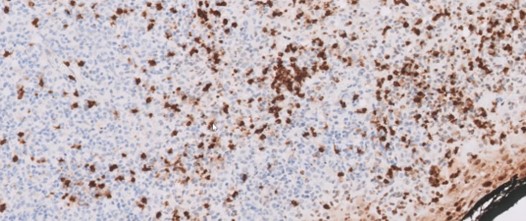
CD56
In situ hybridization for Epstein-Barr virus small-encoded RNA (EBER) was performed on the specimen.
 Meet our Residency Program Director
Meet our Residency Program Director
