“Diagnoses of OPLL are rising globally,” saidKee Kim, UC Davis Health neurosurgeon and the senior author of the review. “There are a variety of OPLL surgical treatments with different approaches. This review will help surgeons choose the best one for the case they are treating.”
Ossified posterior longitudinal ligament diagnosis and symptoms
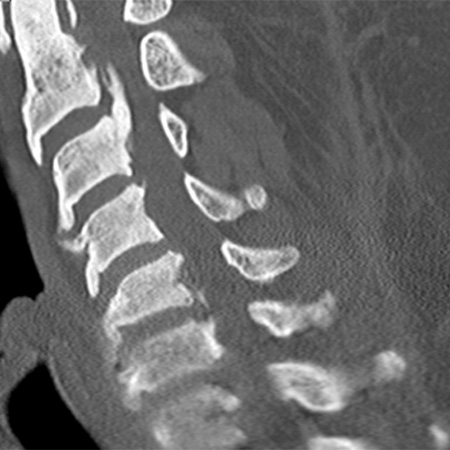
Side view of cervical spine CT showing a large OPLL at the upper part of the spine causing spinal cord compression.
Posterior longitudinal ligamentis a band of tough, fibrous tissue that supports and protects the spine. Ossification calcifies the ligament into a bony structure and leads to OPLL.
OPLL symptoms include pain, numbness and tingling in the hands. As it progresses, OPLL can result in nerve and spinal cord compression (myelopathy). This compression may lead to walking issues and difficulty with bowel and bladder control.
Medical imaging such as X-ray and MRI can help diagnose OPLL and inform the treatment plan. Current treatments range from pain and anti-inflammatory medication to surgery to decompress the nerves and spinal cord.
Flowchart to guide spine surgeons treating OPLL
Surgical decompression is the gold standard once myelopathy develops in OPLL.
The authors present a surgical decision algorithm that integrates various factors, including:
Spinal alignment
How much of the spinal canal is filled by the ossified ligament
Whether the spinal cord can adequately shift away from pressure
“Understanding how OPLL presents and progresses is fundamental to providing a tailored, patient-specific approach to management,” said Freddie Rodriguez Beato. Rodriguez Beato is a UC Davis neurosurgery resident and the first author of the review.
Surgical decompression is the gold standard once myelopathy develops. The review breaks down the different surgical options to relieve this pressure on the spinal cord. It presents a helpful decision-making flowchart that guides spine surgeons with options that include:
Anterior (front-of-neck) surgery: This surgery allows surgeons to remove the bone pressing directly on the spinal cord and improve spinal alignment. It is often used when the bone growth is large or when the spine is curved forward (kyphosis). However, it has a higher chance of complications, like swallowing problems or spinal fluid leakage.
Posterior (back of the neck) surgery: This type of surgery includes laminectomy — the removing of the bony arch of the vertebrae. It is a safer option for patients with multilevel disease and a naturally curved (lordotic) spine. The surgery creates more room for the spinal cord by allowing it to shift backward. Usually, fusion — the linking of two or more bones — is also performed to stabilize the spine and prevent OPLL progression. Another posterior option islaminoplasty, a non-fusion option to decompress the spinal cord for select patients.
Combined surgery may be needed for complex cases — especially when there is severe narrowing or deformity.
Future of OPLL technologies and treatments
The review highlights the growing role of imaging tools, such as the K-line, canal-occupying ratio and dynamic radiographs. These tools help tailor surgical plans to patient anatomy and alignment.
UC Davis neurosurgery residents Jose Castillo and Freddie Rodriguez Beato.
Looking ahead, the review identifies robotics and augmented reality as promising technologies for enhancing precision in cervical (neck) OPLL surgery. Early data suggest high accuracy in screw placement and improved visualization during decompression. Cost and integration barriers persist.
“There is a need to work on the optimal integration of these new tools into the surgical management of OPLL,” commented UC Davis neurosurgery resident Jose Castillo. Castillo is the corresponding author of the review.
The other authors on the review are Muhammad Sulman, Omar Ortuno and Khadija Soufi at UC Davis School of Medicine.